
Miscarriage management has evolved from routine surgical curettage toward less invasive, patient-centered options. One technique at the center of this shift is Manual Vacuum Aspiration (MVA). But should it be preferred over other approaches? The answer depends on clinical context, patient priorities, and resource setting.
🧠 What is Manual Vacuum Aspiration (MVA)?
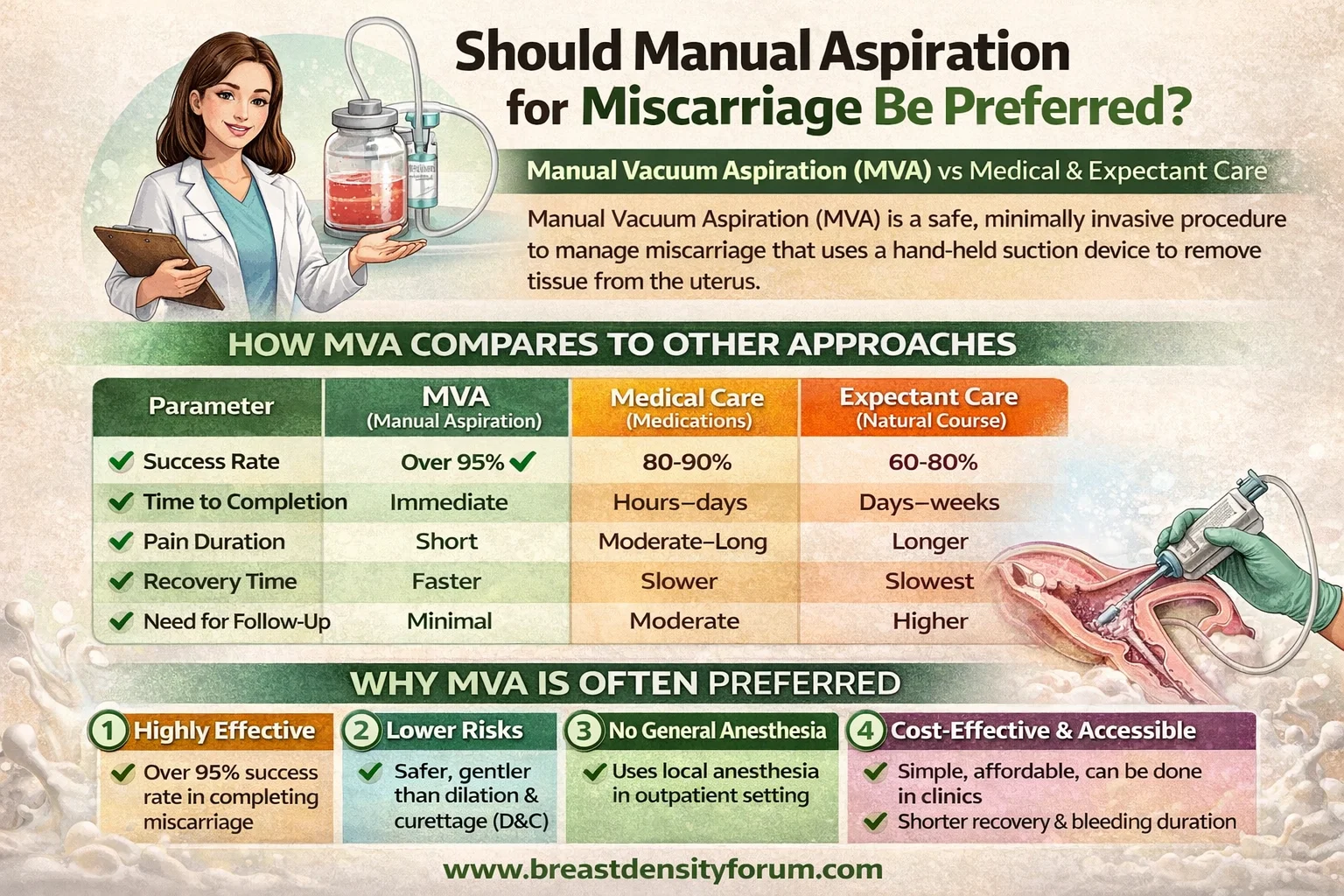
MVA is a safe, minimally invasive procedure that removes pregnancy tissue from the uterus using a hand-held suction device. It is typically performed:
- In early pregnancy loss (usually ≤12–14 weeks)
- Under local anesthesia
- In outpatient or clinic settings
⚖️ Management Options After Miscarriage
There are three standard approaches:
1) Expectant Management (Wait & Watch)
- Natural passage of tissue
- No intervention initially
- May take days to weeks
2) Medical Management
- Medications such as Misoprostol (± Mifepristone)
- Induces uterine contractions
3) Surgical Management
- MVA or Dilation and Curettage (D&C)
✅ Why MVA Is Increasingly Preferred
1) High Effectiveness
- Success rates >95–99% for complete evacuation
- Immediate resolution compared to waiting or medications
2) Lower Complication Risk (vs D&C)
- Less cervical trauma
- Lower risk of uterine perforation and intrauterine adhesions
3) No General Anesthesia Required
- Usually done with local anesthesia
- Safer for patients with comorbidities
- Faster recovery and discharge
4) Cost-Effective & Accessible
- Minimal equipment
- Suitable for low-resource settings and outpatient clinics
5) Better Patient Experience (for many)
- Predictable timing
- Less prolonged bleeding than expectant/medical options
📊 How MVA Compares
| Parameter | MVA | Medical (Misoprostol) | Expectant |
|---|---|---|---|
| Success Rate | Very high | High (but variable) | Moderate |
| Time to Completion | Immediate | Hours–days | Days–weeks |
| Pain Duration | Short | Moderate–long | Variable |
| Bleeding Duration | Shorter | Longer | Longest |
| Need for Follow-up | Minimal | Moderate | Higher |
⚠️ When MVA May NOT Be Preferred
MVA isn’t universally superior. Alternatives may be better when:
- Patient prefers non-procedural care (medical/expectant)
- Very early incomplete miscarriage likely to resolve naturally
- Limited trained providers for MVA
- Infection or hemodynamic instability requiring different management
🧬 Guideline Perspective
Leading bodies like World Health Organization and American College of Obstetricians and Gynecologists emphasize:
- All three options are acceptable
- Choice should be individualized
- MVA is preferred over D&C when surgical management is indicated
🧍♀️ Patient-Centered Decision Making
The “best” option depends on:
- Emotional readiness (immediate vs natural process)
- Access to care
- Pain tolerance
- Cultural preferences
- Prior medical history
🔥 Key Takeaways
- MVA is often the preferred surgical option due to safety, speed, and cost advantages
- It is not universally superior to medical or expectant management
- The optimal choice is personalized, not one-size-fits-all
🩺 Final Verdict
👉 Yes—Manual Vacuum Aspiration is generally preferred when a procedure is needed, especially over D&C.
👉 However, it should be offered alongside medical and expectant options, ensuring informed patient choice.





Leave a Reply