
Introduction
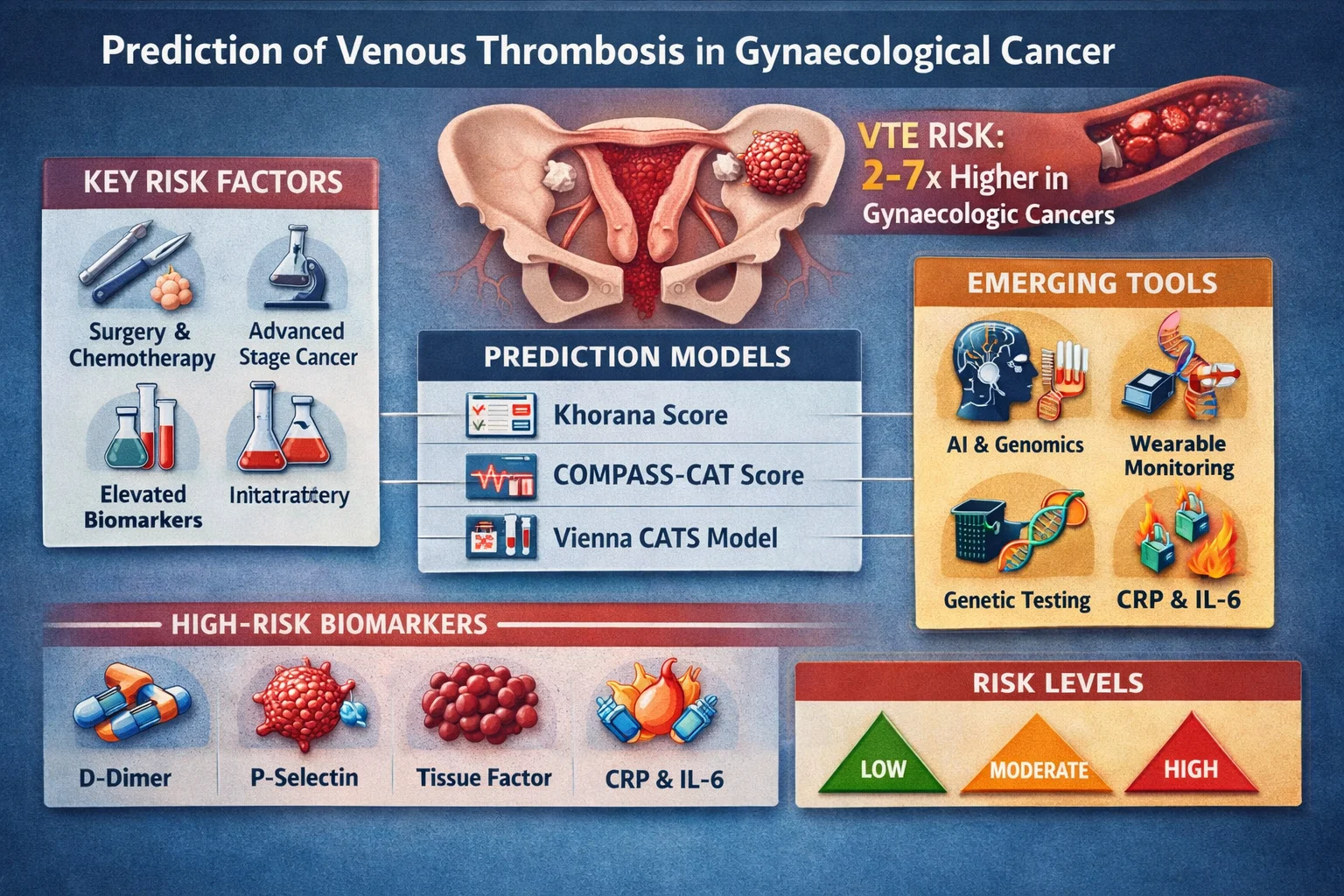
Venous thromboembolism (VTE)—encompassing deep vein thrombosis (DVT) and pulmonary embolism (PE)—is a major cause of morbidity and mortality in patients with gynaecological malignancies. Women with ovarian, endometrial, and cervical cancers face a 2–7× higher risk of thrombosis compared to the general population. Early prediction is therefore not just academic—it directly impacts survival, treatment continuity, and quality of life.
Pathophysiology: Why Gynaecological Cancers Increase VTE Risk
The risk of thrombosis in cancer is classically explained by Virchow’s triad:
- Hypercoagulability: Tumor cells release procoagulants (e.g., tissue factor, cancer procoagulant)
- Endothelial injury: Surgery, chemotherapy, and radiotherapy damage vascular lining
- Venous stasis: Pelvic masses, ascites, immobility, and lymphadenopathy impair flow
Ovarian cancer, in particular, shows the highest thrombotic burden due to high tumor load and inflammatory cytokine activity.
High-Risk Gynaecological Malignancies
| Cancer Type | Relative VTE Risk | Key Factors |
|---|---|---|
| Ovarian cancer | Very High | Advanced stage, ascites, bulky disease |
| Endometrial cancer | Moderate–High | Obesity, surgery |
| Cervical cancer | Moderate | Radiotherapy, pelvic vessel compression |
| Vulvar cancer | Lower | Surgical immobility |
Established Risk Prediction Models
1. Khorana Score (Most Widely Used)
The Khorana Score is a validated tool used across oncology:
Parameters:
- Site of cancer (high-risk sites score higher)
- Platelet count >350,000/µL
- Hemoglobin <10 g/dL
- Leukocyte count >11,000/µL
- BMI ≥35 kg/m²
Limitations in gynaecology:
- Underestimates risk in ovarian cancer
- Does not include surgery or biomarkers
2. COMPASS-CAT Score
The COMPASS-CAT score improves prediction by including:
- Anti-hormonal therapy
- Cardiovascular risk factors
- Recent hospitalization
- Central venous catheter
Advantage: Better discrimination in solid tumors, including gynaecological cancers.
3. Vienna CATS Model
The Vienna Cancer and Thrombosis Study model incorporates biomarkers:
- D-dimer levels
- Soluble P-selectin
Clinical relevance: Moves toward personalized risk stratification.
Biomarkers in Thrombosis Prediction
Key Predictive Biomarkers
- D-dimer → Elevated levels strongly correlate with VTE risk
- P-selectin → Reflects platelet activation
- Tissue factor-bearing microparticles → Tumor-driven coagulation
- Inflammatory markers (CRP, IL-6)
Emerging research suggests combining biomarkers with clinical scores significantly improves predictive accuracy.
Imaging & Screening Approaches
Routine screening is not universally recommended, but targeted approaches include:
- Doppler ultrasound in high-risk postoperative patients
- CT scans detecting incidental pulmonary embolism
- Surveillance in advanced ovarian cancer
Surgical and Treatment-Related Risk Factors
Surgery (Major Contributor)
- Pelvic debulking procedures
- Lymphadenectomy
- Prolonged operative time
Chemotherapy & Targeted Therapy
- Platinum-based chemotherapy
- Anti-angiogenic agents (e.g., bevacizumab)
Other Factors
- Central venous catheters
- Hormonal therapy
- Immobility
Emerging Technologies in Prediction
1. Artificial Intelligence (AI) Models
AI-driven risk prediction integrates:
- Electronic health records
- Imaging data
- Genomic profiles
These models outperform traditional scores in early validation studies.
2. Genomic & Molecular Profiling
Research is exploring:
- Factor V Leiden mutation
- Prothrombin gene mutation
- Tumor-specific coagulation signatures
3. Wearable Monitoring
Early-stage innovation includes detection of:
- Reduced mobility patterns
- Subclinical physiological changes
Risk Stratification Framework (Practical Approach)
Low Risk:
- Early-stage cancer
- No additional risk factors
Intermediate Risk:
- Chemotherapy
- Mild biomarker elevation
High Risk:
- Advanced ovarian cancer
- High D-dimer
- Postoperative state
Prevention Based on Prediction
Pharmacological Prophylaxis
- Low molecular weight heparin (LMWH)
- Direct oral anticoagulants (DOACs)
Mechanical Methods
- Compression stockings
- Intermittent pneumatic compression
Duration
- Extended prophylaxis (up to 4 weeks post-surgery in high-risk cases)
Key Clinical Takeaways
- VTE risk in gynaecological cancer is multifactorial and dynamic
- Traditional models like the Khorana Score need supplementation
- Biomarkers and AI are shaping the future of prediction
- Personalized thromboprophylaxis is the ultimate goal
Conclusion
Prediction of venous thrombosis in gynaecological cancer has evolved from simple scoring systems to multidimensional risk modeling incorporating clinical, biochemical, and technological inputs. The future lies in precision thromboprophylaxis, where each patient’s risk is dynamically assessed and managed—minimizing both thrombosis and bleeding complications.









Leave a Reply